Dear Friends
The Retina Surgeon blog has now moved to the Society for Clinical Ophthalmology website:
http://www.clinical-ophthalmology.com/index.php?option=com_content&view=category&id=82&Itemid=84
OR go to http://www.clinical-ophthalmology.com/
Click on Practitioners
Click on Members Forum in the left frame
Click on Retina Surgery on the submenu.
Direct video upload is not available at the moment, but will be online within the next few days. For now if you could please email me your video either by email to somprasad@gmail.com or by clicking on the mail link on the site, I will get it uploaded.
You can start posting text comments immediately.
Best wishes
Som
Sunday, 28 June 2009
Friday, 19 June 2009
Moving base
Dear All,
Thanks for your support with this blog, it has been a great experience that over 30 colleagues have been following this blog within a few days of starting it, and visitors have grown steadily after that. Your interest has inspired me to seek a wider platform and this blog will soon be moving to the website of the Society for Clinical Ophthalmology.
http://www.clinical-ophthalmology.com/
Please visit this site, and consider joining, it is a vibrant forum, and I believe that joining forces with this Society, will increase the relevance of this blog, and enable better interaction.
Do join, and contribute, the new site will (as we develop it) allow memebers to not only upload comments, but start thier own discussions and upload thier own videos for comment and discussion.
See you at the Society for Clinical ophthalmology website.....
Au Revoir
Som
S Prasad
Thanks for your support with this blog, it has been a great experience that over 30 colleagues have been following this blog within a few days of starting it, and visitors have grown steadily after that. Your interest has inspired me to seek a wider platform and this blog will soon be moving to the website of the Society for Clinical Ophthalmology.
http://www.clinical-ophthalmology.com/
Please visit this site, and consider joining, it is a vibrant forum, and I believe that joining forces with this Society, will increase the relevance of this blog, and enable better interaction.
Do join, and contribute, the new site will (as we develop it) allow memebers to not only upload comments, but start thier own discussions and upload thier own videos for comment and discussion.
See you at the Society for Clinical ophthalmology website.....
Au Revoir
Som
S Prasad
Saturday, 2 May 2009
Video Setup
This question is often asked, what is the best way to get high quality ophthalmic surgical video?
1. Firstly, always leave the recorder running, as interesting things happen suddenly, and turning on the recorder after that mises the key event! These days with large capacity hard disk recorders, I leave it running through the whole operating list - and if nothing of interest occurred, then one can simply wipe the track andrerecord over it the next day!
2. Camera- currently the Sony 3 chip (EXWAVE HAD) cameras still seem to be the best. There are a few new HD cameras out, which are both very expensive, and till most venues get facilities to project HD, maynot be worth the investment
3. Link, Firewire from camera direct to recording device is best - the feed should go straight to the recorder & output from recorder to your TV monitor (not the other way round), A Composite video link, probably delivers similar quality (if your camera doesn't have firewire output)
4. Recorder - I am currently using a hard disk recorder from Datavision. This has 250GB removable drives, so you can record a few days surgery on on disk, take it out - take it to your office/home where you can copy files to PC/Mac and select the bits you want to keep. The rest are deleted. If you have a couple of spare disks, then you can be recording on the next one, whilst sorting the content of the first - so a sort of cycle goes on. Beware of recording direct to DVD, as this is already compressed to mpeg, and whilst output looks good, once you have edited (and sometimes redited more than once), there is loss of quality - the editing software basically tries to decompress the footage, and once you have edited it, recompress it, so every editing cycle has a depreciating effect on quality. Also some hard disk recorders actually compress to mpeg as they record (The Sony medical grade hard disk recorder records as mpeg), what you want is a recorder which records as a native DV stream (Datavision does that) or a relatively lossless format such as AVI - great for mac users as they are already set up to handle DV, but PC users (like me!) can still access the quality if they have the correct software - I use Adobe Premiere CS4, which allows me to import DV files directly and renders them well after editing, although if I play these DV files directly (say through Windows Media Player), the quality is rubish! But once imported into Adobe Premiere - quality is great! Codecs are a dark art which I do not fully understand - but I am here merely trying to explain what works for me (and maybe will for you).
5. Software - If you have an academic connection (Hony Lecturer, whatever), or even a child in full time education, you maybe able to get software on educational prices, which are much cheaper than market rates. I am told (unconfirmed) that Apple UK, if you ring them and say you are a NHS doc who teaches medical students, will give you a discount upto 15% - I haven't tried this being a pC use, but for some of you that may be worth trying.
6. Archiving - this is the biggest problem - Video files are huge - an if You have yaers of them, then you need terabytes of space - that is a separate topic on which I will try to post in the future!
Best Wishes
Som
1. Firstly, always leave the recorder running, as interesting things happen suddenly, and turning on the recorder after that mises the key event! These days with large capacity hard disk recorders, I leave it running through the whole operating list - and if nothing of interest occurred, then one can simply wipe the track andrerecord over it the next day!
2. Camera- currently the Sony 3 chip (EXWAVE HAD) cameras still seem to be the best. There are a few new HD cameras out, which are both very expensive, and till most venues get facilities to project HD, maynot be worth the investment
3. Link, Firewire from camera direct to recording device is best - the feed should go straight to the recorder & output from recorder to your TV monitor (not the other way round), A Composite video link, probably delivers similar quality (if your camera doesn't have firewire output)
4. Recorder - I am currently using a hard disk recorder from Datavision. This has 250GB removable drives, so you can record a few days surgery on on disk, take it out - take it to your office/home where you can copy files to PC/Mac and select the bits you want to keep. The rest are deleted. If you have a couple of spare disks, then you can be recording on the next one, whilst sorting the content of the first - so a sort of cycle goes on. Beware of recording direct to DVD, as this is already compressed to mpeg, and whilst output looks good, once you have edited (and sometimes redited more than once), there is loss of quality - the editing software basically tries to decompress the footage, and once you have edited it, recompress it, so every editing cycle has a depreciating effect on quality. Also some hard disk recorders actually compress to mpeg as they record (The Sony medical grade hard disk recorder records as mpeg), what you want is a recorder which records as a native DV stream (Datavision does that) or a relatively lossless format such as AVI - great for mac users as they are already set up to handle DV, but PC users (like me!) can still access the quality if they have the correct software - I use Adobe Premiere CS4, which allows me to import DV files directly and renders them well after editing, although if I play these DV files directly (say through Windows Media Player), the quality is rubish! But once imported into Adobe Premiere - quality is great! Codecs are a dark art which I do not fully understand - but I am here merely trying to explain what works for me (and maybe will for you).
5. Software - If you have an academic connection (Hony Lecturer, whatever), or even a child in full time education, you maybe able to get software on educational prices, which are much cheaper than market rates. I am told (unconfirmed) that Apple UK, if you ring them and say you are a NHS doc who teaches medical students, will give you a discount upto 15% - I haven't tried this being a pC use, but for some of you that may be worth trying.
6. Archiving - this is the biggest problem - Video files are huge - an if You have yaers of them, then you need terabytes of space - that is a separate topic on which I will try to post in the future!
Best Wishes
Som
Monday, 27 April 2009
Central detachment with myopic hole in extreme myopia
Gentlemen (& ladies),
I did an extreme myope -18 D, phakic with a posterior central detachment and a macular hole. Careful peripheral indented search showed no other holes. I thought I had induced a PVD, but on injecting dilute Triamcinolone realised that there was a very thin sheet of adherent vitreous still there, this was very resistant to come off, and had to be scraped off with a Tano Diamond dusted scraper. Yasou Tano has shown these cases in the past at various meetings, so I had an idea of what needed doing. Having cleared the vitreous and adherent hyaloid to the equator (at least), I decided to do a mid periphereal retinotomy to flatten the retina and then used brilliant peel (blue)under air hoping to stain ILM and remove it. PFCL fill after retina is flat under air, but when I put contact lens on to try and focus on ILM, I just could not get it to focus! Tried to peel ILM through BIOM view - I think with partial success. Laser to retinotomy and an area of 'suspicious' retina peripherally, then direct PFCL to silicon oil exchange. Let us see how she does.
I will try to make the time to edit the video and post it on my blog over the next few days - so watch this space
Som
I did an extreme myope -18 D, phakic with a posterior central detachment and a macular hole. Careful peripheral indented search showed no other holes. I thought I had induced a PVD, but on injecting dilute Triamcinolone realised that there was a very thin sheet of adherent vitreous still there, this was very resistant to come off, and had to be scraped off with a Tano Diamond dusted scraper. Yasou Tano has shown these cases in the past at various meetings, so I had an idea of what needed doing. Having cleared the vitreous and adherent hyaloid to the equator (at least), I decided to do a mid periphereal retinotomy to flatten the retina and then used brilliant peel (blue)under air hoping to stain ILM and remove it. PFCL fill after retina is flat under air, but when I put contact lens on to try and focus on ILM, I just could not get it to focus! Tried to peel ILM through BIOM view - I think with partial success. Laser to retinotomy and an area of 'suspicious' retina peripherally, then direct PFCL to silicon oil exchange. Let us see how she does.
I will try to make the time to edit the video and post it on my blog over the next few days - so watch this space
Som
Sunday, 29 March 2009
Odd submacular lesion with fibrosis
This right eye was initially treated with a haemorrhagic PED in early 2007, presenting with a vision of 6/24. Three Avastin injections were given at 6 weekly intervals, and things settled nicely with vision varying between 6/18 and 6/12 on subsequent visits. The last injection was September 2007.



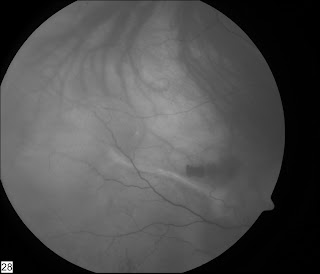


Things remained stable till Feb 09, when she came back with a new complain of seeing a 'blob' in her central vision in her right eye.
Vision was still 6/18
Ant Seg - unremarkable, no cells in her vitreous.
Ant Seg - unremarkable, no cells in her vitreous.
This is her colour fundus photo:


Red Free pictures


She has a clear history of Flourescien allergy, so we couldn't do one.
IR photo:

Her early ICG is shown

Late ICG


Early ICG movie
Mid-phase ICG movie
Late ICG movie
Other eye had PDT some years ago for a fibrovascular PED and settled to a vision of 6/36, been stable for 5+ years.
Any idea about diagnosis? Management?
Wednesday, 25 March 2009
Another 25g Retinal detachment video
Another video showing proper technique to overcome 'weaknesses' of 25g technology.
A good chandelier light and extensive use of deep indentation, means that surgical goals can be achieved, even with relatively flexible instruments.
A good chandelier light and extensive use of deep indentation, means that surgical goals can be achieved, even with relatively flexible instruments.
10th Antwerp VR course 2009
Just got back from Antwerp, excellent meeting as usual in it's 10th edition.
Big play on air tamponade only for macular hole with 3 day face down posturing. I've done a few caes like this with mixed results, anyone else tried this?
The gauge wars continue - 25, 23 or 20? Different people propunding the virtues of one system over the other. What is the outside diameter of a 20g Trocar cannula system for transconjunctival surgery? Must be 19 gauge, if 20g instruments go through the cannula? Will have to look this one up.....
Som
Sunday, 15 March 2009
Inducing a PVD
Usually it is easy to induce a posterior vitreous detachment, but some times the posterior hyaloid face can be very resistant to coming off...
Here is one such case, after trying all the usual manouvres which failed, I decided to 'stain' the vitreous with triamcinolone and then mechanically peel the posterior hyaloid face till I could develop the plane of separation. Once tha was achieved, engaging and pulling up the posterior hyaloid face with the ocutome was easy.
Here is one such case, after trying all the usual manouvres which failed, I decided to 'stain' the vitreous with triamcinolone and then mechanically peel the posterior hyaloid face till I could develop the plane of separation. Once tha was achieved, engaging and pulling up the posterior hyaloid face with the ocutome was easy.
Humour - have a laugh for a change!
The Medical Profession Speaks Out On The Financial Bail-Out Package
The allergists voted to scratch it, and the dermatologists advised not to make any rash moves.
The gastroenterologists had sort of a gut feeling about it, but the neurologists thoughtthe administration had a lot of nerve, and the obstetricians felt they were all laboring under a misconception.
The ophthalmologists considered the idea shortsighted; the pathologists yelled,"Over my dead body!" while the pediatricians said, 'Oh, Grow up!'
The psychiatrists thought the whole idea was madness, the radiologists could see right through it,and the surgeons decided to wash their hands of the whole thing.
The internists thought it was a bitter pill to swallow,and the plastic surgeons said, "This puts a whole new face on the matter."
The podiatrists thought it was a step forward, but the urologists felt the scheme wouldn't hold water.
The anesthesiologists thought the whole idea was a gas; and the cardiologists didn't have the heart to say no.
In the end, the proctologists left the decision up to the assholes in Washington.
The allergists voted to scratch it, and the dermatologists advised not to make any rash moves.
The gastroenterologists had sort of a gut feeling about it, but the neurologists thoughtthe administration had a lot of nerve, and the obstetricians felt they were all laboring under a misconception.
The ophthalmologists considered the idea shortsighted; the pathologists yelled,"Over my dead body!" while the pediatricians said, 'Oh, Grow up!'
The psychiatrists thought the whole idea was madness, the radiologists could see right through it,and the surgeons decided to wash their hands of the whole thing.
The internists thought it was a bitter pill to swallow,and the plastic surgeons said, "This puts a whole new face on the matter."
The podiatrists thought it was a step forward, but the urologists felt the scheme wouldn't hold water.
The anesthesiologists thought the whole idea was a gas; and the cardiologists didn't have the heart to say no.
In the end, the proctologists left the decision up to the assholes in Washington.
Wednesday, 11 March 2009
25g vitrectomy for retinal detachment
I was asked to review a paper for one of the journals on a large series (300+) of 25g transconjunctival vitrectomies. This brought back the arguments for and against this technique to the fore.
25G techniques have been blamed for the flexibility of instruments, the percieved inability to do peripheral work, and in the past for poor light. The light issue has long been sorted by modern sources such as the Photon. The flexibility of instruments, whilst real, can be overcome by changing technique. For instance when 'cleaning' a hole near the ora (very peripheral), traditionally one has the eye in a very tilted position to access the break. However, if you keep the eye flat - and use indentation to bring the area of interest to the vitrector, this problem is solved.
Here is a video clip of a round hole - very near the ora serrata being cleared of vitreous. Eye is flat, tndentation is used to bring the area of the hole to the cutter, thus avoiding the need to tilt the eye and providing a very controlled, very peripheral vitrectomy.
25G techniques have been blamed for the flexibility of instruments, the percieved inability to do peripheral work, and in the past for poor light. The light issue has long been sorted by modern sources such as the Photon. The flexibility of instruments, whilst real, can be overcome by changing technique. For instance when 'cleaning' a hole near the ora (very peripheral), traditionally one has the eye in a very tilted position to access the break. However, if you keep the eye flat - and use indentation to bring the area of interest to the vitrector, this problem is solved.
Here is a video clip of a round hole - very near the ora serrata being cleared of vitreous. Eye is flat, tndentation is used to bring the area of the hole to the cutter, thus avoiding the need to tilt the eye and providing a very controlled, very peripheral vitrectomy.
Monday, 9 March 2009
Laser - from where?
I've been doing a bit of reading about how lasers came to be realised as a tool for the multitude of applications it is used for.
As retinal specialists, we use lasers all the time - in clinics and in the operating theatre.
We've all read about the introduction of opthalmic lasers, but ever wondered where lasers originated...
The clue is Albert Einstein of e=mc2 fame. Besides the theory of relativity, he has many other great ideas to his name. Einstein predicted lasers in 1917!
http://www.aps.org/publications/apsnews/200508/history.cfm
As retinal specialists, we use lasers all the time - in clinics and in the operating theatre.
We've all read about the introduction of opthalmic lasers, but ever wondered where lasers originated...
The clue is Albert Einstein of e=mc2 fame. Besides the theory of relativity, he has many other great ideas to his name. Einstein predicted lasers in 1917!
http://www.aps.org/publications/apsnews/200508/history.cfm
Vitreous base shaving
Ensuring a near complete excision of vitreous base is made much easier with the use of triamcinolone staining. Visulaisation can be further enhanced by using the light pipe as an indentation instrument, as the light nicely transilluminates the kenalog crystals in the vitreous base.
Sunday, 8 March 2009
What am I reading?
Ever wondered about the competency of sutureless incisions for vitrectomy? Well the answer may be in this recent rticle in the American Journal of Ophthalmology.
It seems that a bevelled 25g incision is most competent of the sutureless incisions - however the sutured incisons are still the most secure.
It seems that a bevelled 25g incision is most competent of the sutureless incisions - however the sutured incisons are still the most secure.
Vitreo-macular traction
I used to find diagnosing a Vitreo-macular traction very difficult before the advent of routine OCT. OCT has really enhanced our understanding of the retinl pathology, and 3D rendering can show the pathology even better.
VMT shown clearly on OCT here:

I offerred this patient surgery rather than laser or intravitreal injections and he did very well.
A 3D rendering of VMT -
Drainage of SRF through the tear
Internal drainage of subretinal fluid through the retinal tear in a fresh retinal detachment using a 25g system. As the air comes in the retina flattens nicely. This is a clip from 5 years ago, when the 25g light sourcses were not very bright, but current light sources are both brighter and provide a wide field of illumination.
Follow Blog
Welcome to all the new visitors - If you are wondering how to keep track of the blog posts, why not click on the 'follow' button to the right.
If you are wondering waht this is - a good help file is here
If you are wondering waht this is - a good help file is here
Friday, 6 March 2009
Technical
Colleagues,
I have used two methods to post videos on this blog:
1. Upload to Blogger - these are the videos which appear witha an orange blogger icon in the lower right area
2. Microsoft Silverlight - maybe offers better quality?
For a comparison
See this post - where both formats are available
Retina Surgeon: Does a Wiess ring signify a complete or near complete PVD?
Which do you prefer? It is an important question, as a surgical discussion is best being video based, however image quality, accessebility - ease of download and viewing and similar usability factors are very important
Lets have your thoughts so we can develop the blog accordingly
Best wishes
Som
I have used two methods to post videos on this blog:
1. Upload to Blogger - these are the videos which appear witha an orange blogger icon in the lower right area
2. Microsoft Silverlight - maybe offers better quality?
For a comparison
See this post - where both formats are available
Retina Surgeon: Does a Wiess ring signify a complete or near complete PVD?
Which do you prefer? It is an important question, as a surgical discussion is best being video based, however image quality, accessebility - ease of download and viewing and similar usability factors are very important
Lets have your thoughts so we can develop the blog accordingly
Best wishes
Som
Completely sutureless combined phaco and pars plana vitrectomy
I'm a great fan of sutureless surgery, and have been using sutureless 25g technology for the majority of my vitrectomy procedures since 2003. Of course the later introduction of 23g & then 20g sutureless systems brought in other possibilities...but let's leave that story for another day.....
When doing combined phaco and vitrectomy surgery, even with a 2.85 mm phaco clear corneal incision, I have routinely put a stitch into the corneal incision before going to the post segment procedure, as otherwise, I would sometimes loose the AC during peripheral indentattion whilst completing the peripheral vitrectomy and internal search.
The introduction of sub 2mm phaco technology has solved this problem. Theoretically, the most secure corneal wound is square, and a 1.6-1.8mm wide corneal incision which is of a similar length gets to this theoretical ideal.
So now, the procedure is:
1. Place an inferotemporal 25G cannula in the pars plana and plug it.
2. Do a bimanual microincision phaco using 2x 1.6 mm incisions
3. Implant a microincision lens using wound assisted technique through a sub 2 mm incision
4. Place the infusion line into the preplaced 25g cannula
5. Place two superior 25g ports
6. Complete pars plana vitrectomy (and associated procedures)
7. Remove 25g cannulas
Voila...done
Here is a video of a combined phaco, vity for mac hole case:
When doing combined phaco and vitrectomy surgery, even with a 2.85 mm phaco clear corneal incision, I have routinely put a stitch into the corneal incision before going to the post segment procedure, as otherwise, I would sometimes loose the AC during peripheral indentattion whilst completing the peripheral vitrectomy and internal search.
The introduction of sub 2mm phaco technology has solved this problem. Theoretically, the most secure corneal wound is square, and a 1.6-1.8mm wide corneal incision which is of a similar length gets to this theoretical ideal.
So now, the procedure is:
1. Place an inferotemporal 25G cannula in the pars plana and plug it.
2. Do a bimanual microincision phaco using 2x 1.6 mm incisions
3. Implant a microincision lens using wound assisted technique through a sub 2 mm incision
4. Place the infusion line into the preplaced 25g cannula
5. Place two superior 25g ports
6. Complete pars plana vitrectomy (and associated procedures)
7. Remove 25g cannulas
Voila...done
Here is a video of a combined phaco, vity for mac hole case:
Steps 1 to 5 are as above, then you can see the posterior hyaloid being detached and complete vitrectomy with vitreous base shave using indentation being done. After ILM peel a FAX (Fluid air exchange) is done which finishes with direct drainage from the hole - allowing the hole to close on the table- air is left in as tamponade.
Then 25g ports are removed - and in spite of agressive indentation and peripheral vitrectomy during the posterior segment procedure, the AC remains sealed, deep and well formed.
Thursday, 5 March 2009
can you push back Vit from ant to post segments effectively?
Following blunt trauma this girl presented with vitreous in the AC - formed vitreous - also a GRT (Giant Retinal Tear). At surgery, I thought that getting the vitreous out of the way in the AC - could be a good idea - so after instilling some Kenalog into AC to highlight Vit, I tried injecting into AC to push vit back into PC - did it work? - Watch the video and comment...
Sunday, 1 March 2009
Interactive discussion
Welcome to everyone who has joined over the last few days.
Please add comments to posted cases, and post your own cases so that the interaction is lively and meaningful.
If you have any problems posting do get in touch and I can help. Email link
Please add comments to posted cases, and post your own cases so that the interaction is lively and meaningful.
If you have any problems posting do get in touch and I can help. Email link
Next steps in the oil in AC case
So having not succeeded in controlling his intraocular pressure medically and the iris still being up against the endothelium, there was little choice but to go back to the operation theatre... Making two paracentecis, the AC was reformed using a Rycroft cannula on BSS, an inferior PI was created - see video-
I resisted the temptation to remove oil from the AC, as in the past when I have tried to do so, the oil from the post segment keeps coming forward, and I didn't want to loose tamponade, as the patient was still in the first week of a Giant Retinal Tear repair. He postured face down for 24 hours after this, and the oil in the AC went back to the posterior segment, and his intraocular pressure remained normal and his anterior chamber remained deep. 8 weeks later, I removed his silicon oil via a pars plana approach and his retina remains attached - mission accomplished!
Question: Should I have made an inferior PI at his primary surgery? This is always done for an aphakic eye, but in phakic/pseudophakic/combined IOL vity sil oil cases I have not done this usually?
Thoughts?
I resisted the temptation to remove oil from the AC, as in the past when I have tried to do so, the oil from the post segment keeps coming forward, and I didn't want to loose tamponade, as the patient was still in the first week of a Giant Retinal Tear repair. He postured face down for 24 hours after this, and the oil in the AC went back to the posterior segment, and his intraocular pressure remained normal and his anterior chamber remained deep. 8 weeks later, I removed his silicon oil via a pars plana approach and his retina remains attached - mission accomplished!
Question: Should I have made an inferior PI at his primary surgery? This is always done for an aphakic eye, but in phakic/pseudophakic/combined IOL vity sil oil cases I have not done this usually?
Thoughts?
Monday, 23 February 2009
Oil in AC
Here is someone who I treated for a GRT, pseudophake with an Acrysof len in, so no anticipated ant seg problems. Having sorted his retina out, proceeded to a direct PFCL to OIl exchange, everything went swimmingly, till right at the end - some oil made it's way through the zonules into the AC. You see a sign, the iris is suddenly not sitting on the IOL , but billowed forward!
Should I have done something more at that stage? Who knows, I decided to close up and posture patient face down - hoping to let the oil go back into the posterior chamber...
Did it work - Heck
5 days later patient has an iris plastered to the corneal endothelium, and running pressures over 50 inspite of maximal medication...
What should one do now?
Should I have done something more at that stage? Who knows, I decided to close up and posture patient face down - hoping to let the oil go back into the posterior chamber...
Did it work - Heck
5 days later patient has an iris plastered to the corneal endothelium, and running pressures over 50 inspite of maximal medication...
What should one do now?
Sunday, 22 February 2009
Discuss your surgical techniques
Gentlemen and Ladies,
A lot of the meetings and journals we attend/read concenterate on 'new' treatments and techniques. Basic training in surgical technique is left to a 'apprenticeship' with one's trainer and osmosis from others together with evolution of technique through experience. I propose to discuss the basic surgical tecniques involved in various cases using video clips in this blog and invite others to do so. The format should be a video clip highlighting some problems/difficulties faced, and then to invite others to comment, or give on own views on how these could have been avaoided / better dealt with.
This should not only give those starting out in VR surgery a rich experience, but also cross- fertilise ideas amongst those of us who are more experienced.
I find that the best way of learning surgery, or improving one's technique is by watching your own surgical video. This is an extension of the same principle, by letting others watch your surgery here, you can benefit from others ideas about how to improve your surgery. If you prefer to stay anonymous - send your short write up and video clip to me and I will post it without any identifiable details
You can upload videos directly to the posts (they are hosted on Google Video). If you have any trouble, you can send the video to me, and I can upload it for you. The most practical way of sending across large video files is to use a service such as YouSendIt (free for files under 100 MB). If you are files are larger than this, use a program such as 'Windows Movie Maker' (free in Windows), to compress it for download.
If you still have queries about how to do this, please feel free to email me.
Let's give it a try and see how it pans out.
Best Wishes
Som
A lot of the meetings and journals we attend/read concenterate on 'new' treatments and techniques. Basic training in surgical technique is left to a 'apprenticeship' with one's trainer and osmosis from others together with evolution of technique through experience. I propose to discuss the basic surgical tecniques involved in various cases using video clips in this blog and invite others to do so. The format should be a video clip highlighting some problems/difficulties faced, and then to invite others to comment, or give on own views on how these could have been avaoided / better dealt with.
This should not only give those starting out in VR surgery a rich experience, but also cross- fertilise ideas amongst those of us who are more experienced.
I find that the best way of learning surgery, or improving one's technique is by watching your own surgical video. This is an extension of the same principle, by letting others watch your surgery here, you can benefit from others ideas about how to improve your surgery. If you prefer to stay anonymous - send your short write up and video clip to me and I will post it without any identifiable details
You can upload videos directly to the posts (they are hosted on Google Video). If you have any trouble, you can send the video to me, and I can upload it for you. The most practical way of sending across large video files is to use a service such as YouSendIt (free for files under 100 MB). If you are files are larger than this, use a program such as 'Windows Movie Maker' (free in Windows), to compress it for download.
If you still have queries about how to do this, please feel free to email me.
Let's give it a try and see how it pans out.
Best Wishes
Som
Thursday, 19 February 2009
Does a Wiess ring signify a complete or near complete PVD?
Conventional teaching has been that the visualisation of a Wiess ring implied a PVD (complte or near complete), however surgically when you go into an eye with a well seen PVD, you can often even then, induce a PVD within the posterior pole. Does this mean that the presence of a Wiess ring, is not a predicator of a PVD?
In this patient a Wiess ring was present and is visible at the start of the vitrectomy as a 3/4 circle in mid vitreous. However stndard suction technique to lift the posterior hayloid face able to demonstrate formation of a PVD.
Does this mean that presence or absence of PVD pre-op indeed has no real influence on surgical planning? Or indeed presnce of Wiess ring is not an indicator of PVD, and hence the risk stratification for patients re retinal tears etc may need tobe rethought?
A Higher quality video should be availabale here - if I can figure out how to make it work!
Subscribe to:
Comments (Atom)


